My CIDP Symptoms Development Timeline Progression from year-2000 until now 2026 (Updated)

I was not quite sure what but something was wrong with my muscle movement around year 2000 (at age 54 years) and actually had my first EMG (Electromyography and nerve conductive study) 2002: I was told I had Peripheral Neuropathy, nerve issues in extremities of limbs, caused by stress. However, five years later I became convinced that what was happening was not anything to do with stress nor normal aging. As it turns out I was right and the following is a timeline of my symptoms as I view them since then. Underlying all of the complaints is that they feel strange and impossible to understand. They are difficult to put into words so that a neurologist can understand them and even CIDP specialists do not comprehend some of the symptoms I have had. For example, the feeling (“sensory” response) that my whole body is vibrating and the muscles everywhere, including inside by eyes, my whole face and even brain, rolling like waves is totally beyond the reality of most. Only when the waves or muscle bubbling (twitch-like but not strictly twitching) became visible as "fasciculations" especially in the legs (a “motor response”) more than a year later did my neurologist start taking me seriously. Also by this stage I had already had a serious (almost total) loss of reflex in my knees.
My first nerve conduction study (NCS) October 8, 2002 (aged 56-years) was "pristine" albeit I reportedly had "very high amplitude sensory responses". I underwent this first NCS because I felt something was wrong including a left leg and foot that very occasionally would suddenly begin to drag. April 18, 2008 (aged 62-years), nerve conduction studies by my principal doctor were "suggestive of axonal neuropathy" and CIDP was mentioned but it was reported by that doctor "A" that he did "not have great electrodiagnostic evidence of a primary demyellinating lesion". A second NCS opinion at another hospital (doctor "Tarn") four months later, August 5, 2008, was suggestive of "sensory more than motor polyneuropathy of most likely a demyelinating nature" (but no conduction block was reported). Depite these written reports that demyelination was suspected my principal doctor "T" report March 13, 2009 to my family doctor did not even mention this critical fact on nerve demylination and wrote that "he doesn't have anything serious" and other comments totally dismissive of my complaints. Then over a year later later on May 05, 2010 my condition was revised by my principal doctor to "exceedingly mild CIDP". For more details and my analysis of my nerve conduction studies, click on this link
Although progression from my apparent onset of symptoms at around aged 55 to definitive diagnoses in 2011 aged 65-years took ten years, most of my significant new symptoms have the same pattern of coming on quite suddenly and unexpectedly .
Is my CIDP eyeball / eye Centered: At first my mind and body struggles to overcome the mysterious new issue – and it can be traumatic. When my eyeballs (especially when my eyes are closed or resting) went out of control March 2009 (with wild feeling of eye waves, vibration, shudder & tremor) it started over a weekend and remained severe for ten days: I felt like I could fall deeply into a psychotic stupor from which I would never recover. It took a week of fretting before I allowed myself to sleep accepting that I would be waking. When told of the complaint, my neurologists looked at me blankly and in complete disbelief! Eyeball / eye fasciculations continue 2022 as a huge troubling symptom and since 2009: It has NEVER been relaxing to close my eyes for rest. My eye / eyeball issues seem very complicated as both peripheral and/or autonomic nerves could be the cause. I also have a whole-body vibration, muscle-bubbling feeling that began early and indeed I believe is a precursor to visible fasciculations and the beginning of the pain for me. (To be clear my fasciculations is NOT a muscle twitch) An important side-note is that my definitive CIDP diagnosis was championed by a Neuro-Ophthalmologist after other neurologists told me nothing was wrong for eight years! Now in 2022 I have learned that eyeball fasciculations are recognized by experienced neurologists as a serious issue that occurs in other neurological conditions like MS and MG (also prevalent in epilepsy)! Indeed there is an eye-dominant variant of GBS/CIDP called Miller Fisher syndrome but I apparently do not have that!
My life-threatening breathing issue which began 2012 started and developed in a period of about two months although at first I could not believe that this was CIDP at work. Fortunately, the breathing issue subsided and is no longer a threat by January 2018. Importantly, it seems after a while my body adapts to the new symptom as per the saying "it gets worse before it gets better" - this is a noticeable short-term pattern that has emerged with most of my symptoms over the years living with CIDP, although this may be that I adjust and learn to cope with the new issue. I have found that the worsening of symptoms over the long term began in my legs and moved upwards through my arms shoulders and in the last year my neck and head.
Entering 2015 (aged 69-years), I transfer to the CIDP Clinic at Toronto General Hospital. I have had no IgG for a year and getting worse! I have new challenges as the CIDP has moved upwards affecting my hands and arms - the progression seems rapid as usual but hopefully the new IVIG infusions will reverse this. Ending 2015 my condition does not seem to have improved and now continuous pain has become a big problem with seemingly no position helping to reduce it. My three leading complaints entering 2016 (aged 70 years) were major pain, more upper-body involvement, breathing issues and apparent autonomic "body control system" involvement (sweating, blood pressure, temperature, mood, digestion etc). While these issues persist, by April 2017 my body has definitely adjusted and I feel there is more stability with the effect of the maintenance IVIG and my ability to manage my CIDP symptoms (except unstoppable pain). My breathing issue has almost completely resolved but still now in 2018 (aged 72-years) and my CIDP doctors say nerve conduction studies show I am stable on the neuromuscular front but this is not allaying my fear that this is faulty. My number one issue by far is my increasing excruciating spreading pain. My neuro-pain seems not directly mitigated by the IVIG therapy and I am afraid of taking drugs for pain. My next ranked further issues are: fasciculations (which also exacerbate pain), rapid loss of ability to maintain ANY still position (including sitting), loss of balance and unsteadiness (loss of body and limb motion control). Also unresolved: extreme sensitivity to cold and sudden onset of dizziness/near fainting (even at rest). December 2018 NCS results show no change on the neuromuscular side. By early 2019 I have experience continued symptom spread through my shoulders, neck to head (with eye issues worsening). Following my adverse reaction to IgG mid-2020 I have taken a turn very much for the worst - November 03, 2020: Doctors believe I am having an allergic reaction to CUVITRU or IgG, and as a result I am off all IgG. I judge my overall health at less than 20% of the the pre-diagnosis level entering 2021, knowing I have very uncertain days ahead.
My Life-threatening CIDP 2021 a Decade gone and No-one Listening after IgG?: August 2021 I am becoming concerned and, after two visits to emergency for head, face, eye and weird brain issues I feel I have a life-threatening situation. I have been examined by more than ten doctors and I have even told my main doctors directly of my belief that my life is threatened. But the doctors do not seem to grasp the urgency of my situation (or more likely disagree with my assessment). I am even consulting doctors abroad: October 9, 2021 in Portugal on the advice of an specialist in autoimmune diseases, I did comprehensive immune-system blood tests (Euro €1900). I also consulted a neurologist specializing in head issues including cerebral vascular diseases and neuroimmunology and had a head MRI (Euro €400) October 18, 2021. I judge my overall health in October 2021 at about 5% of the the pre-diagnosis level. The Portugal neurologist consultations produced valuable result. December 13, 2022, after twenty months off all CIDP drugs, I am officially discharged from the CIDP program as I am "doing very well" and my CIDP is stable ! .
July 16, 2024 a my dentist discovers I have "Eagle Syndrome" caused by an elongated styloid process and calcified stylohyoid ligaments around the jaw. Eagle Syndrome could explain some of head/ face symptoms as the syndrome effects the cranial nerves (and cranial #10 vagus nerve with autonomic nerve system connections), carotid arteries and jugular vein. See panoramic x-ray showing my elongated styloid process. Mid-2025 I have begun to grasp the huge significance of cranial nerve involvement in my MADSAM CIDP - indeed, quite shocked in retrospect at the apparent lack of concern for my facial pain complaints demonstrated by my CIDP doctors given cranial nerve significance to my case.
{kind=link}
My 2026 Rapidly Deteriorating CIDP symptoms (such as trouble walking, walking wobble, limb pain and weakness) confirmed in a Nerve Conduction Study of December 13, 2025. All historic symptoms are worsening, notably the top ten now May 14, 2026 are listed after my CIDP timeline table below. I am struggling quite a lot to keep mobile and May 22, 2026 receive my first injection of Argenx Vyvgart SC / efgartigimod alfa . .
This page represents a summary timeline of my CIDP events. This website also contains a detailed monthly, or even daily sometimes, of the timeline. You can view a timeline listing of the detailed log pages, with their page links, at the bottom of this page.
Below you will find a summary timeline of development for my CIDP symptoms from year-2000 (aged 54-years) to Jan 2026 (aged 80-years): 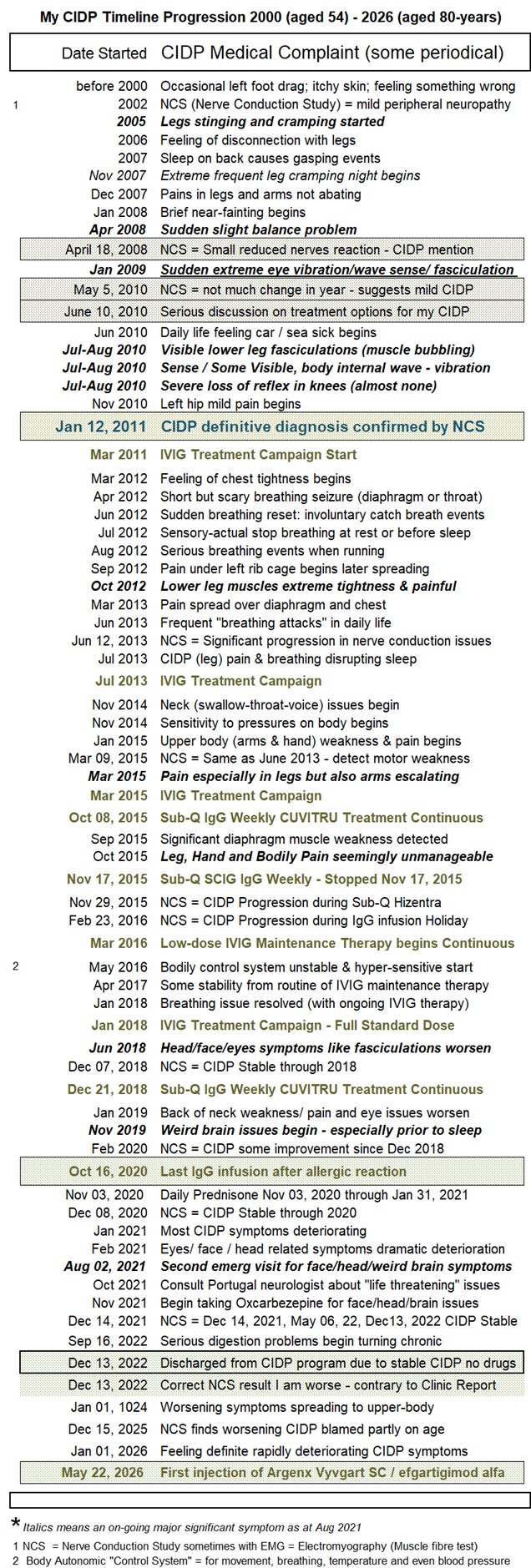
and the chart following shows my Index of the Monthly Severity of my CIDP symptoms 2013-2017 :

UPDATE 2026: All historic symptoms are worsening, notably the top ten in the last year increases in:
• disconnect between my brain and movement
• left leg collapsing at knee, foot and hip
• bodily walking resistance and weakness
• foot and leg wobble / walking instability
• fasciculation (muscle bubbling, waves, vibration and tremor)
• deep-rooted pain in ligaments everywhere
• any beyond average movement causing cramping
• greatly increased cranial issues and neck
• autonomic dysfunction in breathing (breathing hiccups) and bowel movement
• new weird surface skin patchy very painful stinging attacks
My Detailed CIDP Logs: I started logging my CIDP situation from July 2013 when my CIDP doctor asked me to keep notes of my reactions to my first round of IgG therapy. I have continued making notes to this day April 20, 2026 and beyond. You can follow my postings at the following links of listed by timeline date:
> 2013 July: Daily log of 2nd eight-months round of IVIg July 2013 - April 2014
> 2015 March: Log of IVIG impacts March-October 2015
> 2015 October: Log of Sub-Q trial SCIG of Hizentra) Oct 2015
> 2016 March: Log Maintenance Dose IVIg Therapy Mar 2016 though 2018
> 2018 January: Log of clinical trial of Panzyga IVIG Jan-Dec 2018
> 2018 December: Log of Sub-Q Ig Cuvitru Sub-Q Dec 2018 through Oct 2020
> 2020 November: Log transition off IgG after Adverse Reaction Nov 2020
> 2021 February: Log Going-Solo no CIDP Drugs Feb 18, 2021 - July 16, 2024
> 2024 July: Log CIDP vs Eagle Syndrome July 16, 2024 - Dec 2025
> 2026 January: Log CIDP hitting 80 years-old - the End Game from Jan 2026
* Autonomic Nerves Control System" - CIDP or related faulty autoimmune condition has somehow affected my autonomic nervous system of which breathing, digestion / micturition (bowel and bladder), swallowing, eye control (papillary response) is dependent. The early breathing and 2016 temperature (with night sweats) resolved and are no longer a significant issue in entering 202
CIDP Eye Issues Article 2013: “Chronic optic neuropathy in chronic inflammatory demyelinating polyneuropathy: A case report"by Shohei Watanabe1,*, Masanaka Takeda, Tomoko Saito, Akiko Kimuraand Hiroo Yoshikawa. Neurology and Clinical Neuroscience Volume 1, Issue 2, pages 78–81, March 2013. ABSTRACT:. Although some previous reports have suggested optic nerve involvement in chronic inflammatory demyelinating polyneuropathy (CIDP), the clinical course of optic neuropathy has not been well reported. We report a Japanese individual who developed “chronic” optic neuropathy with CIDP. She presented with subacute visual loss of the left eye, and her visual function did not improve until she was treated with two courses of intravenous steroid therapy and seven sessions of immunoadsorption (IA). Although these immunomodulation treatments were carried out 6 months after the onset of visual loss, her visual acuity completely recovered. These findings suggest that optic neuropathy in CIDP patients can show a chronic clinical course, and immunomodulation therapy might be effective against optic neuropathy with CIDP, even when administered during the chronic phase.
CONCEPTS for CIDP Timeline: the stages of cidp, cidp prognosis, early signal, first sign for CIDO, early indications for CIDP, new CIDP patient, initial CIDP symptoms, primary sign CIDP, how to diagnose CIDP, how long does it take for CIPD, how to tell CIDP, what signs signal CIDP, CIDP Progression, the phases of cidp, progress of CIDP, how long does CIDP take, start of CIDP, when diagnosed with CIDP, development of CIDP, how do you get CIDP, contract CIDP, CIDP development steps, is CIDP contagious, CIDP indications, indicator for CIDP, long term CIDP prognosis, log the time for CIDP, record CIDP steps, Chronic Inflammatory Demyelinating Polyneuropathy autonomic neuropathy dysautonomia