My CIDP Nerve Conduction Studies (NCS) Record and Analysis 2002 through 2026 for Chronic Inflammatory Demyelinating Polyneuropathy CIDP
CIDP nerve conduction studies (NCS) + CIDP electro-diagnostic electromyography (EMG) + My Own Personal Analysis of NCS Results

My first nerve conduction study (NCS) October 8, 2002 (aged 56-years) was "pristine" albeit I reportedly had "very high amplitude sensory responses". I underwent this first NCS because I felt something was wrong including a left leg and foot that very occasionally would suddenly begin to drag. April 18, 2008 (aged 62-years), nerve conduction studies by my principal doctor were "suggestive of axonal neuropathy" and CIDP was mentioned but it was reported by the doctor that he did "not have great electrodiagnostic evidence of a primary demyelinating lesion". A second NCS opinion four months later, August 5, 2008, was suggestive of "sensory more than motor polyneuropathy of most likely a demyelinating nature" (but no conduction block was reported). Then almost two years later on May 05, 2010 my condition was revised by my principal doctor to "exceedingly mild CIDP". Now in March 2026 I am finally doing my own analysis of NCS results with the assistance of an excellent team - an EMG Technologist with 30-years experience and her daughter a whiz-kid data analyst. I will shortly be posting the results here.
In 2015 when I was transferred to the CIDP Clinic at Toronto General Hospital (TGH) the Nerve Conduction Studies conclude my "nerve conduction study and needle examination show evidence of demyelinating polyneuropathy affecting the lower limbs (legs)". Motor and sensory studies of median nerve (arms) are normal. Motor studies of left peroneal and tibial nerves (both lower leg) show low CMAP, prolonged distal latencies, and slow conduction velocity. Since a study of left sural nerve (a purely sensory nerve of the lower leg and foot) shows slow conduction velocity. F waves of left median nerve (arm) are normal but prolonged and left peroneal and tibial nerves (both lower leg). Vibration perception thresholds are prolonged in the lower limbs. Needle EMG examination show evidence of denervation potentials in left tibialis anterior and gastrocnemius muscles, normal and vastus lateralis. The nerve conduction study and needle examination show evidence of demyelinating polyneuropathy affecting the lower limbs." Your can view the 2015 NCS report at this link:"NCS-Clinic-Report-CIDPlog-2015-03-09.pdf.
Key Diagnostic Parameters in CIDP
Which is the most important parameter to diagnose CIDP: DML, CV, CMAP, or F latency
- DML (Distal Motor Latency) prolongation in ms: Crucial for identifying distal demyelination, where a DML >50% above the upper limit of normal is a major criterion. Distal Motor Latency (DML) increases (becomes prolonged) in patients with Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)..
- CV (Conduction Velocity) decrease in m per s: Essential for identifying segmental demyelination, requiring a reduction ≥30% below the lower limit of normal. Conduction velocity (CV) decreases (slows down) in patients with Chronic Inflammatory Demyelinating Polyneuropathy (CIDP).
- F-Latency (F-wave) prolongation in ms: Highly sensitive, particularly in early cases or where other studies are normal, as it tests proximal segments and root involvement. F-Latency (F-wave latency) increases (prolongs) in patients with Chronic Inflammatory Demyelinating Polyneuropathy (CIDP).
- CMAP (Compound Muscle Action Potential) in mV: While reduced amplitudes (CMAP) are found in CIDP due to axonal loss, the diagnosis of demyelination is based on conduction velocity slowing, DML, F-wave latency, or abnormal temporal dispersion. The Compound Muscle Action Potential (CMAP) amplitude typically decreases for patients with CIDP.
v Motor Nerve Parameter Charts:
Distal Motor Latency (DML) For diagnosing Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), no single parameter is considered "most important" because the diagnosis relies on demonstrating demyelination across a combination of these values. You can view the demyelination values required in a table at this link In my NCS analysis I am most interested in the trends over time, as I delve further into the data.
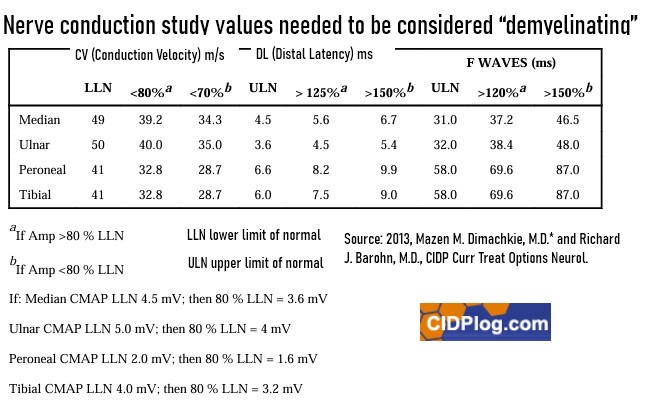{kind=link}
However, Distal Motor Latency (DML) is statistically noted as the parameter least likely to contribute to false positives in some cohorts. So below are my results for Distal Motor Latency between 2002 and 2025:.

CV (Conduction Velocity): Also my results for motor nerve velocity between 2008 and 2025:

F-Latency (F-wave) prolongation: My results for F-Latency (F-wave study) prolongation in ms between 2008 and 2025:

CMAP (Compound Muscle Action Potential): My results for CMAP (Compound Muscle Action Potential) in mV between 2002 and 2025:

v Sensory Nerve Parameter Charts:
Sensory Latency: My CIDP doctors tell me that I am 70-80% sensory versus motor nerve involvement with my MADSUM classified CIDP. So below are my results for Sensory Latency between 2002 and 2025:

Sensory Nerves Velocity: Also my results for sensory nerve velocity between 2008 and 2025:

Sensory CMAP (Compound Muscle Action Potential): My results for sensory CMAP (Compound Muscle Action Potential) in mV between 2008 and 2025::

You can view the raw NCS data used to generate the above charts at the following link CIDPlog-NCS-Results-Detail-Spreadsheet-Print-2020-2025.pdf
v My Situation Now 2026 aged 80 years Old - and Perplexed at NCS Inconsistency
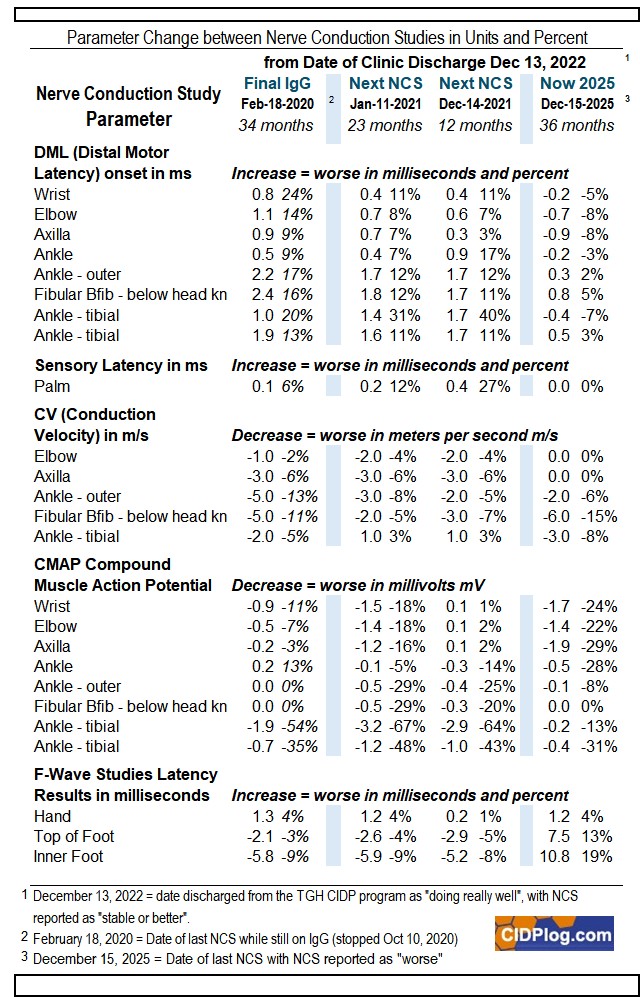
Unconscionable Differences: I began my analysis in early 2026 as I awakened to the realization that I needed more control of my situation as my CIDP doctors seem stymied on what to do with me. In 2022 I posted on this site that I was perplexed as to why December 13, 2022 I was discharged from the CIDP clinic, when I was symptomatically feeling so bad. So, first thing now, is to investigate why the hospital report December 13, 2022 read "nerve conduction studies are stable to better" - when my every-day symptoms were clearly telling me otherwise (For detains see My CIDP log February 18, 2021 - through mid 2024}. Turns out now in April 2026 I am finding contrary results to the official hospital report. Here is my analysis of the related NCS data:
 .
.
You can download a PDF version of this table at the following link NCS-Results-since-Discharge-2020-2025.pdf
» April 2026: I have found unconscionable differences between what I have concluded now April 2026 versus what I have been led to believe in the past three years. Seems I was in deterioration-free-fall December 13, 2022 when the hospital CIDP Clinic report for the NCS of that day read:"nerve conduction studies are stable to better" and the clinical note for NCS read "Improved". Looking at the above data, I cannot find much, if any, evidence to support the CIDP Clinic statements. Indeed, the opposite is true and, rather, the deterioration accelerated that year between NCS done December 14, 2021 and December 13, 2022. Furthermore, the data does offer support to my reporting rapid spread of negative CIDP symptoms upwards from legs to arms. I am very worried about apparent axonal loss measured by CMAP - with its highly noticeable decline - which impair my mobility and could affect my central nervous system.
Events both before and after the CIDP Clinic consultation December 13, 2022 were actually quite dramatic and documented in my log at that time at link My CIDP Since Going-Solo without CIDP Drugs February 18, 2021 - July 16, 2024. I was forced to consult doctors in Portugal for both mini-seizures and supra-ventricular tachycardia SVT arrhythmia, when neither the CIDP Clinic or other local doctors failed to act. I also in desperation had my family doctor refer me to new neurologists (although not expert in CIDP). Even the doctor referred by the CIDP Clinic December 13, 2022 for the mini-seizures took six months to contact me too late. On this website I logged: January 29, 2023: Entering 2023 I am far from feeling "doing really well" (my primary CIDP doctor's words). By mid-January I had a very disturbing turn for the worst when I had two critical breathing mini-seizures. In the last two weeks I have also had two instances of sudden onset of rapid pulse. Again, I am finding reason to believe that my brain mini-seizures, arrhythmia and breathing mini-seizures have their root cause in CIDP (potentially via the cranial nerves)†. All of this in addition to my other symptoms that I felt deteriorating: spreading pain, cramping, imbalance, dizziness, increasing weakness, etc
† Cranial Neuropathy in CIDP-2021-01-01.pdf
v Was Nine Years of IgG Immunoglobulin Effective in Preventing My CIDP Progression?
I was on IVIG or SCIG IgG for nine-years and pretty much always felt better when on than off. You can view my logs of how it was for on various pages of this website, and an overview of the period is given at the following link My Summary Assessment of Immunoglobulin IgG IVIG for CIDP 2011 until 2020. One can surmise from the above NCS parameter trend charts that the infusions did mostly stabilize my CIDP while under treatment.
This is also largely supported in a more detailed breakdown of periods (except for the CMAP parameter). The following table shows the changes in units and percentage for the whole period, the time I attended the TGH CIDP Clinic, and for the 69 months I have received no treatment at all:
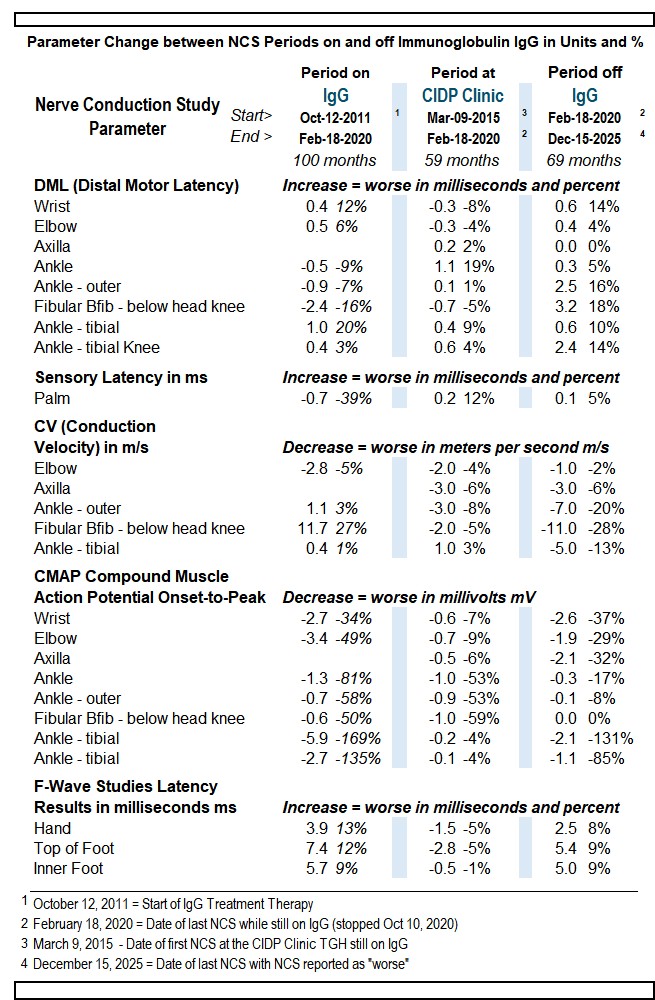
You can download a PDF of the above table here CIDPlog-NCS-Results-for-IgG-2011-2025.pdf
Further evidence of IgG effectiveness is in the period immediately after stopping IgG, which shows a very high rate of progression in all parameters. From a NCS standpoint, I clearly did much better on IgG than off with no CIDP drugs. This fact is consistent with the worsening symptoms I reported after February 18, 2020.
This nerve conduction webpage will be updated when I get my next NCS. Meantime:
>Last Dated Log 2026 at this Link.
without
Concepts for My CIDP Record and Analysis 2002 through 2026 of Nerve Conduction Studies (NCS) record for Chronic Inflammatory Demyelinating Polyneuropathy: How to interpret nerve conduction studies for neurological deceases like Electrodialysis-pre-diagnosis electromyography (EMG), electrode , CIDP patient analyses own nerve conduction studies over 20 years